What is shoulder instability?
Instability is defined as the symptom patients refer when the shoulder slips in its normal position. Shoulder joint instability may be caused by laxity, where it is difficult to keep the shoulder in site for alteration of bone and/or periarticular tissue development. Dislocation of the shoulder is often caused by trauma or microtraumas.
An unstable shoulder can dislocate (the femoral head completely comes out of its normal lodging, the glenoid of the scapula), subluxate (partial dislocation of the humeral head) or present with pain in specific positions or movements due to abnormal gliding of the femoral head in during sports or work. When dislocation occurs frequently, even after a long period of time, it is called recurrent dislocation.
Why does shoulder dislocation occur?
The shoulder joint is a very special joint compared to the others of the human skeleton. The humeral head, approximately hemispheric in shape, loosely rests on a shallow concave vertical surface 3.5 cm high and 2.5 cm wide. This configuration allows the shoulder to have a wide range of motion in the three directions. However it is subjected to gravity therefore during motion joint stability is dependent on the connective tissues: joint capsule and glenoid labrum, ligaments and muscles with their respective tendons.
Because of its particular conformation and anatomical distribution the shoulder dislocates more frequently in the antero-inferior direction. In these cases tears occur in bone and cartilage, ligament and tendon depending on the amount of the force and direction of the trauma, number of recurrences and individual resistance of the structures enduring stress.
At what age does it most frequently occur?
This pathology has a higher incidence in the second and third decades of life, is more frequent in males than in females and is related to the completion of muscle and joint development as well as to the peak of physical and working activity. However, although rarely, dislocations can occur also in other age groups: infants, adults or even elderly.
How is diagnosis made?
Medical history of the shoulder or of both shoulders, diffused laxity also in other joints (congenital diseases like Marfan’s syndrome generate laxity in all ligaments), the modality (for severe trauma or with no apparent trauma), the frequency, concomitant to specific body movements or positions, are all elements to be considered.
At physical examination the patient must assist the orthopaedic surgeon by performing certain movements and specific manoeuvres to help define certain lesions excluding others which may co-exist. Attention must be paid to the fact that frequently the patient automatically tightens muscles and examination becomes difficult. Physical examination of the shoulder before surgery is useful because under anesthesia the muscles in the limb relax and dislocation can be evaluated better. For a sure diagnosis and to program therapy other instrumental examinations may be performed.
Which are the most appropriate instrumental examinations?
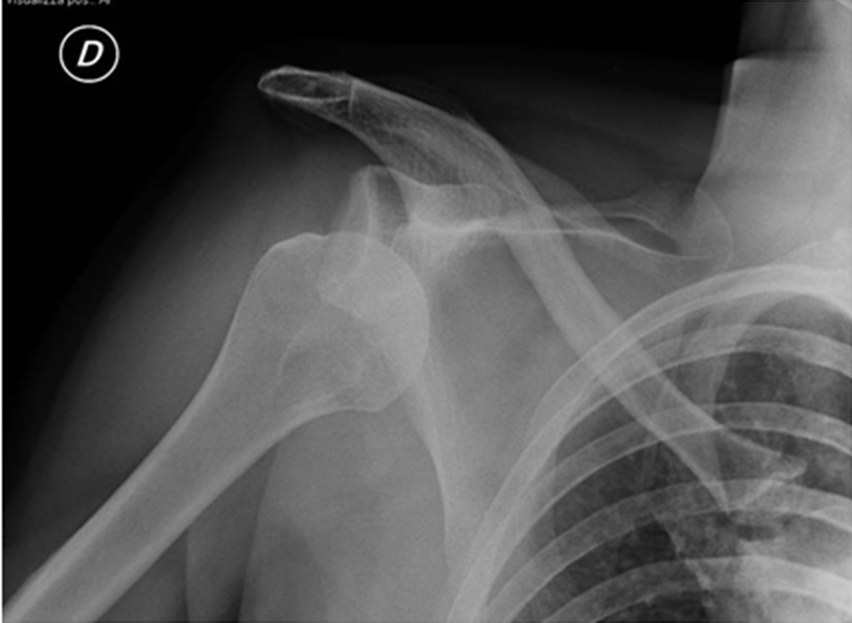
Standard x-rays are necessary prior to shoulder reduction. Examinations useful to confirm diagnosis and for surgical staging are computerized axial tomography (CT) and magnetic resonance imaging (MRI) scans. CT shows conformation, joint relations and possible proximal humerus and glenoid surface bone damage and more specifically if there are fractures or bone fragments. MRI gives more complete information for connective tissue tears and muscle trophism. In selected cases, to obtain a clearer definition and image of the damaged structures and areas adjacent to the joint both CT and MRI can be performed using contrast dye injected directly in the joint.
What treatment options are available?
The treatment of choice after a first dislocation is conservative: reduction, orthopaedic bandaging and after about 4 weeks immobilization, progressive mobilization using elastics is started to strengthen the subscapularis (for anterior instability) or the subspinal (for posterior instability) muscles. If instability persists and should dislocations recur surgery may be considered.
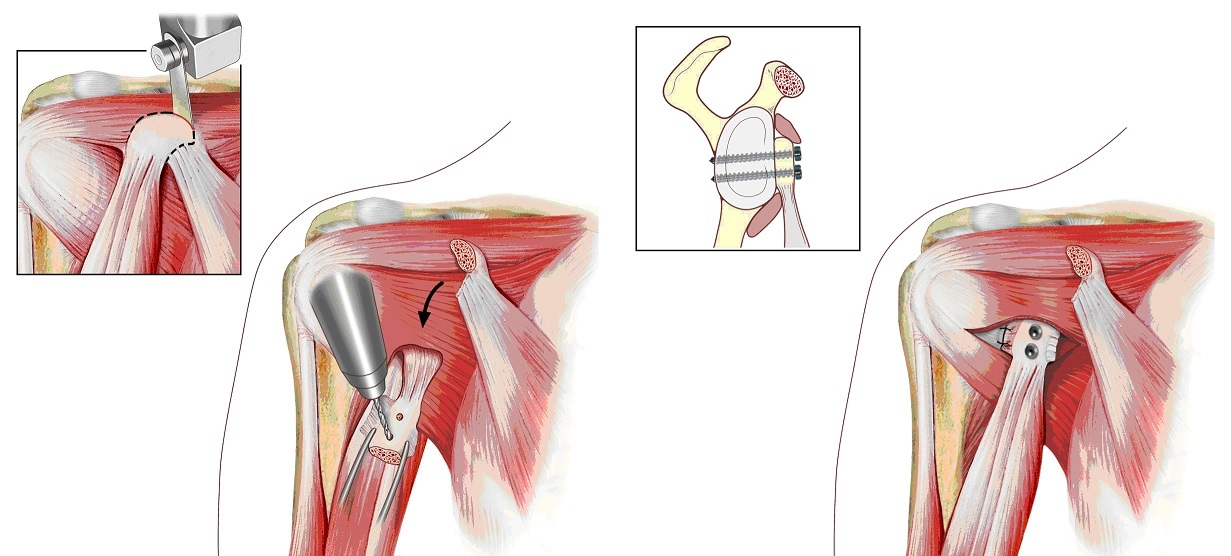
In the past 20 years surgical techniques for shoulder instability have brought about more precise surgery tailored on the specific tears and on the single patients. The decision as to when reparation surgery of the lesions and reinforcement of the capsule (capsulo-muscular plastic surgery) should be performed is taken together with the surgeon. However, at a certain point it is the same patient who feels the need to intervene on a situation of unease no longer tolerable with an everyday working and social life.
The surgical technique chosen depends mainly on: age, frequency of the dislocations or if these are absent, duration of shoulder pain and degree of impediment during sports or working activities, muscle structure, level of weight-bearing during work, sports practiced as professionals or amateurs. It is important to rule out the presence of fractures associated to the dislocation, for this CT or MRI are very useful.
Arthroscopy: what advantages?
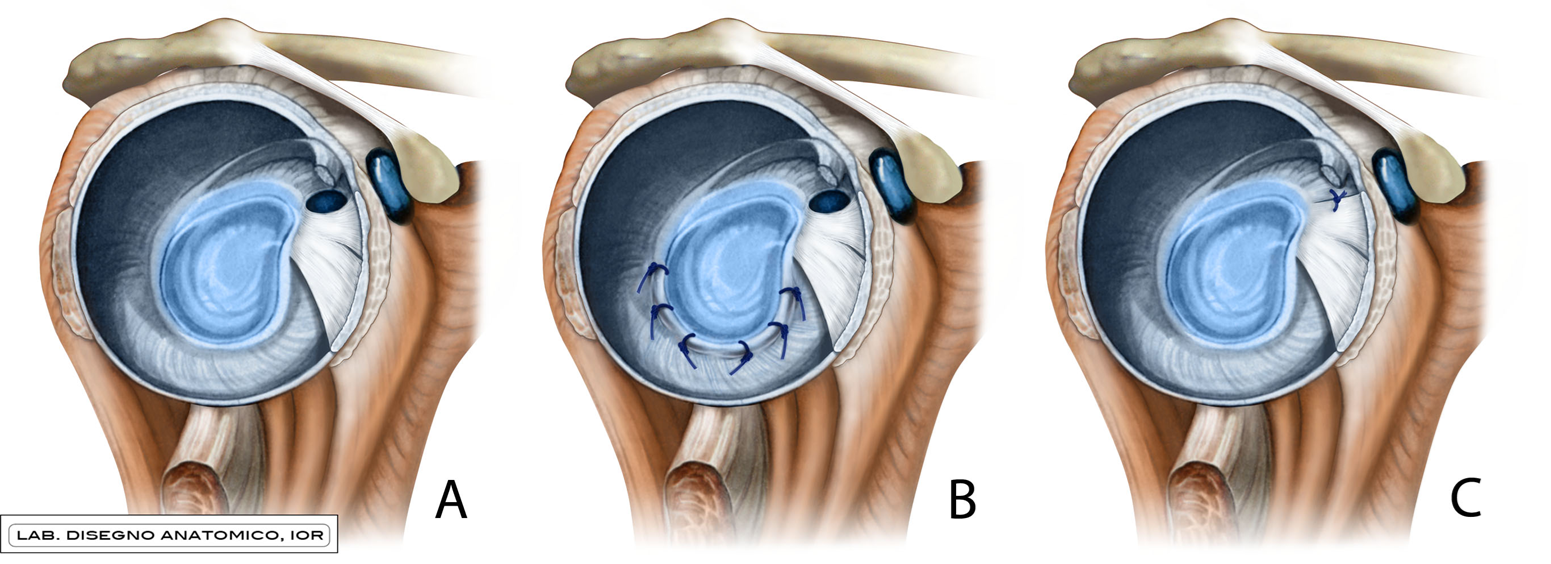
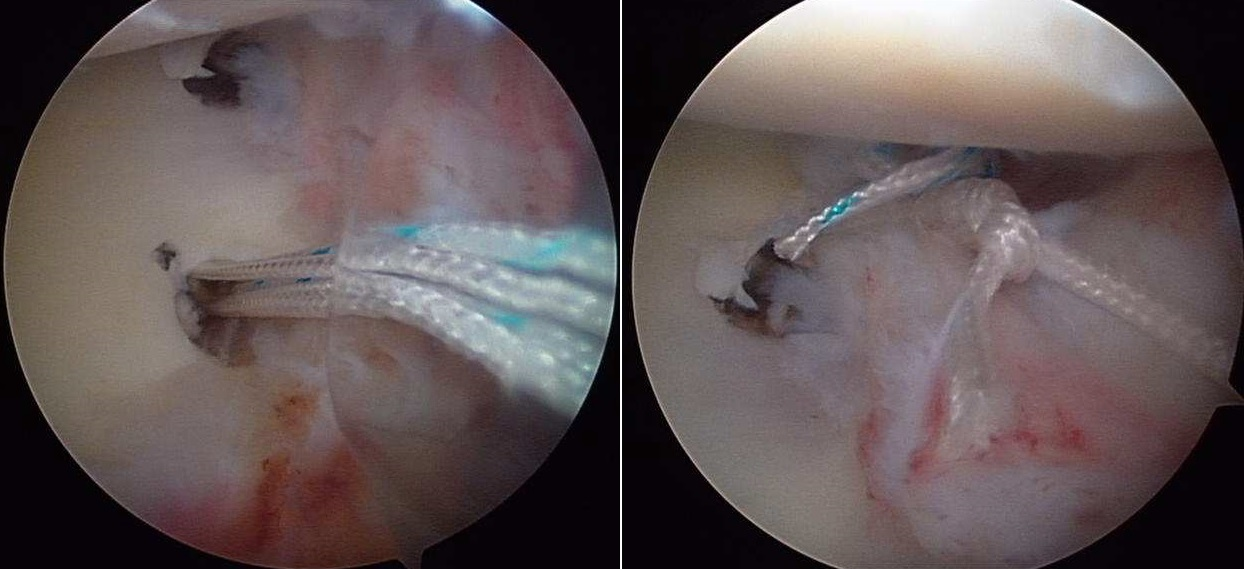
In the past 15 years improvements in arthroscopic techniques (small incisions to access the joint and small instruments controlled by microcameras) have greatly improved results. The advantage of not excising the muscles and the precision in repairing the tears makes this technique suitable for young patients (from 15 to 30 yrs of age), with a limited number of dislocations and with microinstablity. The technique uses “suture anchors” similar to microscrews (in titanium or resorbable polylactic acid) with nonresorbable highly resistant threads that are passed and tied to the joint capsule and to the glenoid labrum to recreate the normal capsular tension.
This surgical procedure is always requires general or combined anesthesia (regional anesthesia with or without deep sedation) and hospitalization for 3 or 4 days. The upper limb is placed in an orthopaedic bandage for 4-5 weeks, then functional rehabilitation of the shoulder is started, first passive and later active, assisted by a physiotherapist, preferably in water, with complete recovery of joint movement after 6-8 weeks.
What happens when the shoulder is not operated?
This question is frequently posed especially by patients with an unstable shoulder but with no dislocations and thus less invalidating. Some elderly patients have shoulder lesions without having had any real traumas, but with a history of heavy working activity or episodes of recurrent dislocations in youth always treated conservatively. These are painful lesions and the decrease in strength varying according to the extension of the lesion. In these cases and in this age group positive results of reparation surgery, are uncertain because of the instability present that was never corrected.
Edited by Enrico Guerra, MD and Marco Nigrisoli, MD
Shoulder and elbow surgery - Istituto Ortopedico Rizzoli, Bologna